Visual Evoked Potential (VEP) Explained
What is Visual Evoked Potential (VEP)?

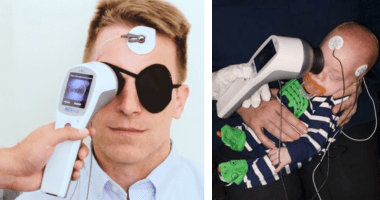
How VEP works
A light stimulus provided by a computer monitor or ganzfeld bowl is received by the retinal cells of the eye. The electric potential travels from the retina to the visual cortex of the brain. Electrodes placed on the occipital lobe record the resulting electrical activity within the visual cortex.
What VEP tells us
Abnormalities in the VEP indicate potential distruptions in the visual pathway. VEP can help to detect the causitive mechanism of visual deficits.
- It is useful as a test of the visual pathway as a whole.
- Normal VEP indicates that visual information is successfully transmitted to the brain’s visual cortex for interpretation.
- Abnormalities may indicate issues with the transmission from the eye to the visual cortex.

VEP testing provides functional and objective data
VEP is a non-invasive measure of the electrophysiological responses of the brain to visual stimuli. VEP testing provides objective and recordable functional information even for non-cooperative, non-verbal, or unconscious patients.
Although imaging technology like MRI continues to advance, VEP is regarded as a valuable tool to help detect occult lesions within the visual pathway, and most especially within the optic nerve.
Why conduct VEP testings?
VEP is an objective test of visual function. Numerous syndromes and anomalies can affect the VEP, including optic neuritis, multiple sclerosis (MS), tumors, traumatic injuries, infections, and toxic agents. Interpretation of the VEP abnormalities can help differentiate between possible types of underlying pathologies.
Clinical Applications of VEP
VEP, as an aid in diagnosis and disease management, is clinically valuable to clinicians in the determination of neurological deficits causing vision issues — even when imaging is unreliable or inconclusive, or when symptoms appear to be subjective only. Likewise, VEP can be used to track functional recovery after an acquired or traumatic neurological event.[44]
VEP testing can therefore be used to assess:
- Misrouting in the optic nerve fibers (e.g. albinism)[43]
- Toxic or nutritional optic nerve dysfunctions[43]
- Optic neuritis suspects (resulting from demyelination e.g. multiple sclerosis)[42]
- Recovery from a range of optic pathway dysfunction[42]
- Cortical blindness due to meningitis or anoxia[42]
VEP testing can also be used to:
- Distinguish between inflammation and other optic neuropathies[42]
- Quantitatively ascertain visual system function and optic pathways due to head trauma[42]
- Help detect orbital tumors compressing the optic pathway[42]
- Monitor for potential optic nerve gliomas in patients with neurofibromatosis[42]
- Monitor cerebral function of patients in operating rooms or intensive care[44]
3 Types of VEP Tests
Different visual stimuli have been designed to produce different types of VEP results. In general, the clinically most used types of VEP testing are pattern-reversal VEP (PVEP or PRVEP), pattern-onset VEP, and flash VEP. Pattern-reversal stimulation is the gold standard for VEP testing, with the most consistent timing and waveform.[45] On the other hand, pattern-onset VEP and flash VEP are more commonly used for patients who cannot fixate such as infants.
Pattern-Reversal VEP
A pattern-reversal VEP (PRVEP) waveform is generated by a phase-reversing checkerboard. The PRVEP waveform contains three peaks of interest: N70, P100, and N155. The P100 is the most robust measure, exhibiting the lowest interpatient and intereye variability as well as high repeatability.[47] Therefore, the robustness and consistency of the PRVEP enable general rules of interpretation and is most commonly used for patients with suspected optic nerve diseases.[43]
Most common indications where PRVEP is used are Traumatic optic neuropathy, optic neuritis, Ischemic optic neuropathies or toxic or nutritional optic nerve dysfunction.[43][46] These conditions are typically characterised by absent PRVEP waveforms, reduced amplitudes ratio (affected/fellow eye), or delayed peak times, with each of the indications helping to identify or confirm a suspected disease.[43]
However, VEP abnormalities are nonspecific, and an adjunctive test of macular function is required. This may include a pattern ERG, mfERG or flash ERG[31] — conducted with the UTAS system or flash ERG[43] with the RETeval® device.
The Pattern-Onset VEP
The pattern-onset VEP waveform is generated by an on-off checkerboard stimulation. The pattern-onset VEP is composed of C1-positive—C2-negative—C3-positive peaks. A core application of pattern-onset VEP is the detection of chiasmal misrouting of albinism in older patients, where this stimulus type is actually required.[45]
It has other applications as well. Similar to flash VEP, pattern-onset is useful when nystagmus is encountered, or when the patient has difficulty fixating (e.g. young children). The VEP standards set forth by ISCEV recognize that while intra-patient variability in flash and patter-onset VEP can be high, nonetheless, inter-ocular comparisons of these waveforms can provide clinically valuable information. This includes the trans-occipital distribution of monocular responses.
The versatile UTAS system can perform pattern-onset testing. However, for most applications, flash VEP can perform analogous testing functionality to that of pattern-onset. In this case, the handheld and portable RETeval device may be a better solution.
Flash VEP
Flash VEP is produced by a white flash generated from a ganzfeld bowl. The waveform represents a sequence of alternating negative and positive readings. The P2 (corresponding to the P100 in the PRVEP) and N2 peaks are the most clinically relevant measures.[44]
The key benefit of flash VEP is that it does not require patient cooperation for fixation/focus and can be used even when the patient is sedated. The flash VEP is, therefore, generally indicated in small children, people with developmental disabilities, or otherwise non-compliant patients.[44]
Flash VEP with the RETeval device can be used to monitor cerebral function even in anesthetized or comatose patients. Half-field stimulation can indicate whether VEP abnormalities stem from a retrochiasmal lesion and thus it is useful in assisting best in the diagnosis of the effects of albinism.[44]
The handheld and portable RETeval device is capable of performing flash VEPs. This is also available with the versatile UTAS device.